Following the introduction of a surgical protocol that leveraged intraoperative imaging with a combination PET-CT scanner to assess the success of head and neck cancer resection, surgeons have used the technology for breast cancer.
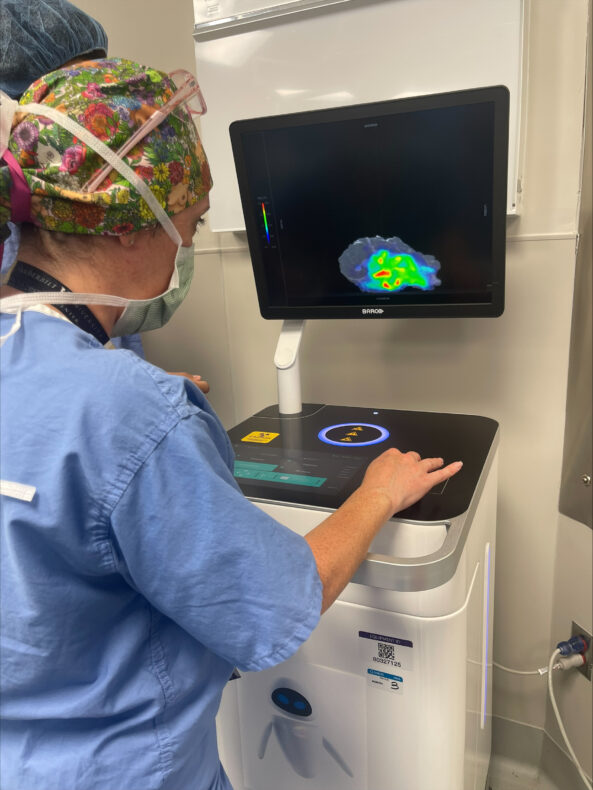
Denise Garcia, MD, uses the Xeos Aura 10 scanner to image a recently excised breast tumor from a patient. The use of the Xeos Aura 10 device ensures the imaging and assessment can be done in the operating room rather than in the pathology lab. (photo by Kyrionna Golliday)
Investigators led by Michael Topf, MD, Associate Professor of Otolaryngology-Head and Neck Surgery, performed the nation’s first surgery using intraoperative PET-CT scanning in September 2025. Now, a surgical team led by Denise Garcia, MD, Assistant Professor of Surgery in the Division of Surgical Oncology and Endocrine Surgery, has applied the technology to successfully resect a breast cancer mass.
“This application of intraoperative PET-CT is proof that countless patients can benefit from the expansion of this novel imaging methodology,” said Garcia. “Our team is proud to apply it to a type of tumor that has not yet been imaged for the purposes of assessing margin status. As our institution expands treatment methodologies to more types of cancer, we can cure more patients and give them peace of mind that their surgery has been completed with precision. This technological advancement underscores the success we’ve had across multiple disciplines in working toward that goal.”
Rapid expansion of intraoperative PET-CT scanning boosts efficiency, offers peace of mind to surgeons and patients alike
With each new application, surgeons are demonstrating that an intraoperative PET-CT imaging protocol can help reduce wait time for results from several days to a matter of minutes and allow surgical teams to know immediately whether they need to continue operating.
During surgery, the patient receives a dose of a radioactive agent that illuminates the cancer tissue in the scanner. Once the tumor is excised, it is placed in a specialized mobile PET-CT scanner called an Aura 10 device, developed and supplied by Belgium-based surgical technology company Xeos. The scanner negates the need to send the specimen to the pathology lab, providing surgical teams with a real-time view and allowing them to quickly determine if the entire cancerous mass was removed.
If any mass remains, the operation continues. If the cancer has been successfully resected, the surgery concludes, and the patient is sent home with peace of mind, knowing they won’t need to return for a follow-up surgery, and with confidence that their surgeons have a precise, immediate look at the results of the surgery. Because patients receive the radioactive agent on the day of surgery rather than in advance, they also receive a lower dose of radiation.
Dan Hannon of Georgia traveled to Vanderbilt Health, where a robotic bronchoscopy was used to retrieve tissue from a hard-to-reach area of the lung. Hannon now has a confirmed lung cancer diagnosis and will begin treatment. (submitted photo)
When Dan Hannon, 72, received guidance to have part of a lung taken out whether nodules were cancerous or not, he wanted a second opinion to see if he would indeed live the rest of his life without a full set of lungs.
After incidentally learning of a suspicious spot in his lungs while getting imaging to diagnose a kidney stone in 2025, he was advised to get his lungs checked. Several months later, he had a diagnostic PET scan under the care of a Georgia pulmonologist near his home in Buford, Georgia.
Some spots “lit up,” indicating metabolic activity, which often means cancer but may be due to infection or inflammation. He went on to get a bronchoscopy, a minimally invasive procedure using a camera on a thin tube to examine his lungs and obtain biopsy tissue.
He and his wife, Janice, learned the areas that were successfully biopsied were benign, but there were two additional areas the physician couldn’t reach.
Thus came the recommendation for an open surgery to remove the undefined tissue for biopsy. It was also advised that Hannon have a sizeable portion of his affected lung removed while still under anesthesia, regardless of the biopsy results.
That didn’t sit well with the couple, so they drove four hours to Vanderbilt Health in Nashville. Their son had been successfully treated for cancer there in the past.
“The prior lack of knowledge of whether I had cancer or not, and being told I should have surgery and get part of my lung cut out — whether it was cancer or not — was very bothersome,” Hannon said. “I decided to get a second opinion. I wanted all the information I could get to make a good decision, and that’s exactly what’s happened.”
Fabien Maldonado, MD, MSc, points out a target lesion easily visible in the image of the lung generated by the cone-beam CT. (photo by Susan Urmy)
At Vanderbilt Health, a new approach to a difficult diagnosis
The Hannons met with Fabien Maldonado, MD, MSc, professor of Medicine and Thoracic Surgery and director of Interventional Pulmonology at the Vanderbilt Lung Institute. Maldonado told them he was pretty confident he could reach those areas for biopsy using robotic bronchoscopy, the standard of care at Vanderbilt University Hospital.
“Robotic bronchoscopy, combined with cone-beam CT, has transformed the way we do things,” said Maldonado, who holds the Pierre Massion Directorship in Lung Cancer Research. “Ninety-five percent of people with lung nodules don’t have cancer, but for the 5% that do, they need to receive a diagnosis and get treatment as soon as possible.
Inside the robotic bronchoscopy advancing lung care
During a robotic bronchoscopy, physicians use a controller to precisely guide a bronchoscopy tube, which is typically smaller and more flexible than traditional tubes. The additional agility allows access into the lung’s harder-to-reach peripheral structures so biopsy tissue can be obtained. A 3D, high-resolution image of the lung obtained through cone-beam computed tomography (CBCT) is displayed on a monitor to guide the interventional pulmonologist’s progress.
At Vanderbilt Health, the four board-certified interventional pulmonologists who do the robotic bronchoscopies have all completed a fellowship and an additional year of interventional pulmonology training before receiving board certification from the American Association for Bronchology and Interventional Pulmonology.
A robotic bronchoscopy at Vanderbilt University Hospital. At center is the robotic arm, with a control console on the left of the interventional pulmonologist. The semicircle above the patient is a cone-beam CT scanner that creates a 3D view of the lung. (Vanderbilt Health)
Oncologist Mohamed Shanshal, MBChB, assistant professor of Medicine, said robotic bronchoscopy significantly improves getting patients the appropriate treatment as soon as possible, reducing their anxiety and improving care.
To expand access to the diagnostic procedure, the Vanderbilt Health Interventional Pulmonology program recently bought two additional robot and CBCT systems, making it one of the largest interventional pulmonology programs in the South. Four state-of-the-art bronchoscopy suites are slated to open later this year.
“This reduces diagnostic uncertainty and helps us move more quickly from suspicion to confirmed diagnosis,” Shanshal said. “Earlier and more accurate tissue diagnosis allows us to initiate treatment sooner, including surgery, targeted therapy, immunotherapy or clinical trials. In lung cancer, timing and adequate tissue for molecular testing are critical to optimizing outcomes.”
Maldonado explained that the Interventional Pulmonology program is a national leader in testing new technologies for safety and results.
“Many new technologies related to lung nodule biopsies have come on the market without any data to prove their benefit,” Maldonado said. “We are doing the randomized controlled trials here to prove whether something new is better than what we’re already doing. We study these technologies carefully and quickly, and within six months to a year, we know if the new is more beneficial and needs to be adopted.”
Cytotechnologist Sanders Murphree, left, and Fabien Maldonado, MD, MSc, view the biopsied tissue under a microscope to ensure it is of suitable quality for the pathologist to make a definitive diagnosis. (photo by Susan Urmy)
From uncertainty to action: What Hannon’s biopsy uncovered
For the Hannons, having the assurance that the robotic bronchoscopy would reach the spots in his lung and offer clearer details about their makeup was important.
“With the help of the robot, Dr. Maldonado was able to get what he needed, and it came back as adenocarcinoma,” Hannon said. “He was awesome when he explained his findings and everything we needed to do.”
Hannon has mucinous adenocarcinoma, a rare, non-small cell lung cancer that accounts for 2-10% of all lung adenocarcinomas and is most often found in the outer regions of the lung.
During a return visit to Nashville in late February, Hannon had a pulmonary function test, and met with Konrad Hoetzenecker, MD, PhD, professor of Thoracic Surgery, who will soon surgically remove the cancerous spots, and with Shanshal, his new oncologist.
“We’ve had a fantastic experience at Vanderbilt, and we’ve got a fantastic team of medical professionals we’re working with,” Hannon said. “We’re prepared for surgery and any future treatment because of the consultations we’ve had with Dr. Maldonado, Dr. Hoetzenecker and Dr. Shanshal. This has given me confidence in what has to happen.”
And as the Hannons move with hope toward healing, they’re looking forward to future cruises and travels to visit family.
A study published in the journal JAMA Surgery demonstrated the benefits of using fluorescence-guided imaging to assess margins in head and neck cancer. Researchers at Vanderbilt University Medical Center found that leveraging data collected both during surgery (in vivo) and after the tumor’s removal (ex vivo) can help guide surgeons in achieving a negative margin in cancer resection.
A margin refers to the areas around the tumor being removed. The desirable outcome is to complete surgery with a negative margin, indicating that no cancer was found at the edge of the resection. A positive margin indicates that cancer cells remain in the tissue, which increases the risk of recurrence and reduces the chance of survival.
To assess those margins, surgeons may use fluorescent agents administered to the patient’s tissue. Systemically infused agents have been shown to differentiate cancerous and healthy tissue with high accuracy.
“Our research found that the use of fluorescence imaging both internally and externally can improve surgeons’ ability to precisely and safely excise tumors,” said Shravan Gowrishankar, MD, a research fellow in the Department of Otolaryngology-Head and Neck Surgery and the study’s first author. “This research seeks to illuminate methods of leveraging fluorescence imaging to achieve negative margins, particularly for deep resections, which often prove difficult.”
This figure illustrates an example of a tumor with two types of margins: mucosal, which surrounds the surface of the tumor, and deep, which is healthy tissue beyond the tumor. Deep margins are more difficult to navigate for surgeons, but fluorescence imaging seeks to change that. (courtesy of researchers)
The researchers defined two classifications of margins: the superficial or mucosal margin refers to the area uninvolved with the tumor but surrounding its surface, while the deep margin refers to the 4 to 5 millimeters of healthy tissue beyond the tumor’s most invasive points, or the depth of normal tissue between the tumor edge and the cut surface of the specimen.
“Currently, it’s easier to achieve negative mucosal margins than deep margins,” said corresponding author Eben Rosenthal, MD, chair of the Department of Otolaryngology-Head and Neck Surgery and Barry and Amy Baker Professor of Laryngeal, Head and Neck Research. “Deep margins aren’t able to be assessed as easily because surgeons must rely on estimation of the distance from the tumor to guide the resection.
“We sought to improve methods of achieving negative margins across the board because estimation isn’t good enough where patient safety is concerned.”
The assessment of deeper margins is further confounded during surgery by tissue retraction and the presence of blood, which can obscure the view of the surgeon. And while autofluorescence — a process by which naturally occurring chemicals in the tissue can absorb light of a particular wavelength and reemit it at a different wavelength — can help surgeons assess mucosal margins, deeper margins are impossible to assess via this process because the light does not penetrate beyond a millimeter.
To assist in ensuring a negative margin in a deep resection, surgeons can use fluorescence imaging techniques. Mapping tumors after resection can provide data on how close the margins are to the surface of the deep resection, and intraoperative in vivo fluorescence imaging can reveal areas of residual disease in the tumor bed. In combination, the information provided by both methods of fluorescence imaging can guide further examination and sampling to help achieve fuller resection of the deep margin.
While both methods in combination are critical to achieving better outcomes in surgery, said Gowrishankar, ex vivoimaging devices have certain advantages over in vivo hardware.
Shravan Gowrishankar, MD
“While the data we get from in vivo imaging is valuable, it’s largely qualitative because of variance in ambient light in the operating room,” said Gowrishankar. “Ex vivo imaging is more precise because we can seal out external light in a controlled environment to measure fluorescence intensity and guide our assessment of deep margins.”
In ex vivo imaging, fluorescence intensity increases the closer the tumor tissue approaches the cut surface of the tumor specimen, and data from this measurement can be used to create a sort of “heat map” measuring the relative depth of the tumor across the entire specimen. By using this imaging technique, surgeons can more precisely detect the reach of cancer cells in the tissue and perform precise resections.
“Mucosal margins are easy enough to detect during surgery without fluorescent agents, but those agents are critical in helping us close the gap with deep margins,” said Rosenthal. “Missed deep margins contribute to the majority of positive margins after resection, which in turn contribute to negative health outcomes for patients. Large-scale adoption of these techniques will have a meaningful impact on the health of patients who undergo surgery to remove cancerous tumors.”
Additional authors from Vanderbilt University Medical Center include:
Jennifer Choe, MD, PhD, assistant professor of Medicine in the Division of Hematology Oncology
Alexander Langerman, MD, SM, FACS, associate professor of Otolaryngology-Head and Neck Surgery
Kyle Mannion, MD, FACS, associate professor of Otolaryngology-Head and Neck Surgery
Aviva S. Mattingly, MD, MS, VTOPS/R25 Research Resident
Sarah L. Rohde, MD, MMHC, associate professor of Otolaryngology-Head and Neck Surgery and division director of Head and Neck Oncologic Surgery
Robert Sinard, MD, FACS, professor of Otolaryngology-Head and Neck Surgery
Hidenori Tanaka, MD, PhD, visiting assistant professor of Otolaryngology-Head and Neck Surgery
Michael Topf, MD, MSCI, assistant professor of Otolaryngology-Head and Neck Surgery.
This research was supported by the National Cancer Institute, part of the National Institutes of Health (grants R01CA279249, R01CA239257, R01CA266233 and R01CA238686).
Fluorescent nanoparticles clearly identified colonic adenomas precursors to colorectal cancer in mice and the formulation should translate to clinical use in humans.