Allison Young is easing the pain for people grieving the lost connections when a loved one dies by providing a place for words left unspoken and milestones that can no longer be shared.
It’s a small phone booth without utility wires or cellular connections nestled along her driveway in East Nashville. The messages are carried by love vibes. Since Young erected the booth two years ago, it has become a sanctuary of solace and garnered attention from local and international media.
She learned about a “wind phone” while she was working on the thesis for her master’s degree, researching alternative grieving methods, and delving into the continuing bonds theory — a concept that it’s okay for people in mourning to maintain connections to loved ones who have died instead of just having to let them go.
The first wind phone was erected in 2010 in northern Japan by Itaru Sasaki, who wanted to talk with his cousin who had died from gastric cancer.
“Since he couldn’t talk to him in person on a regular phone line, he wanted his words to be carried on the wind,” said Young, MS, BSN, RN, a research nurse specialist for clinical trials at Vanderbilt-Ingram Cancer Center. “He lived at the top of a hill right next to the ocean, so there was lots of wind. It was a perfect concept for him. Then unfortunately, four or five months later was when the tsunami hit Japan, the one that killed tens of thousands of people along the northern Japanese coast.”
The tsunami devastated Ōtsuchi, the town where Sasaki lived, with about 10% of its population of 16,000 perishing. Sasaki’s wind phone became the place where grieving survivors went to connect with lost loved ones.
“Now, thousands of people from around the world have made the trek to northern Japan to see the original wind phone,” Young said. “The idea has spread across the entire world. There are wind phones in other places in Asia, in Australia, all over North America, and a ton in Europe as well.”
The “wind phone” allows people a place for words left unspoken and milestones that can no longer be shared. (photo by Donn Jones)
Young put up her wind phone booth in September 2022, then unveiled it to the wider community in February 2023.
“It is dedicated to my paternal grandparents,” she said. “We opened it on the 24th anniversary of my grandfather’s death, and it is dedicated to my grandma who died in 2016. She is the only person I have ever called on it, and I called her the day I defended my thesis.”
Young has received notes from more than 200 people who have visited it. The structure is a circa 1940s actual phone booth. Her father, who is a contractor, helped her set it up by putting a slanted roof over its flat top and weatherproofing it with exterior paint. The booth is soundproof with a privacy curtain.
“There’s a light so that people can use it overnight as well,” she said. “Since I am a nurse, I know what health care hours are like, so I made it available 24 hours a day.”
The door has a sensor to help her keep records of visitors, but there are no cameras or privacy infringements. Visitors are encouraged to park in her driveway because Rosebank is a two-lane road with a narrow shoulder.
The wind phone has been featured in news stories and documentaries, including coverage by NHK, Japan’s public media organization, and by “This American Life,” a public radio program in the United States.
This is a randomized, two-cohort, open-label, phase 3, clinical trial to compare the efficacy and safety of N-803 plus tislelizumab and docetaxel (cohort A) or prior failed Health Authority-approved antiprogrammed death-1 (PD-1) or anti-programmed death-ligand 1 (PD-L1) CPI and docetaxel (cohort B) versus docetaxel monotherapy (cohorts A and B).
For each cohort, enrolled participants will be randomized 2:1 to treatment in the experimental arm or the control arm. For cohort A, the randomization will be stratified by geographical region (North America vs Europe vs Asia vs Other), NSCLC histology (squamous vs nonsquamous), and actionable genomic alteration (AGA) (epidermal growth factor receptor \[EGFR\]/anaplastic lymphoma kinase \[ALK\]/ROS proto-oncogene 1, receptor tyrosine kinase \[ROS1\] vs Other AGA vs No AGA).
For cohort B, the randomization will be stratified by geographical region (Americas vs Asia Pacific \[PAC\] vs Other), NSCLC histology (squamous vs nonsquamous), and actionable genomic alteration (AGA) (Yes vs No).
This year’s Clip In 4 the Cure drew hundreds of participants to Geodis Park for a relay-style team cycling event featuring top Nashville spin instructors and live DJs.
The high-energy fundraiser began in 2022 to raise money for cancer initiatives at Vanderbilt-Ingram Cancer Center and Monroe Carell Jr. Children’s Hospital at Vanderbilt.
Clinicians and patient ambassadors highlighted the impact that the fundraising efforts have on cancer care and research.
This is a multi-center, first-in-human (FIH), open-label, Phase 1a/1b dose escalation and dose expansion study to assess the safety, PK, pharmacodynamics, and antitumor activity of PHST001 monotherapy (Phase 1a) or in combination with chemotherapy (Phase 1b) in adult participants with advanced relapsed and/or refractory solid tumors (including but not limited to CNS tumors in Phase 1a only). In Phase 1b cohort expansions, the study will focus on participants with advanced relapsed and/or refractory ovarian cancer, endometrial cancer, and cholangiocarcinoma. The study's primary objective is to evaluate the safety and tolerability of PHST001 and determine the RP2D (Recommended Phase 2 dose) of PHST001 monotherapy and in combination with chemotherapy as well as assess the anti-tumor activity of PHST001 and chemotherapy in Phase 1b.
This phase II trial tests the addition of venetoclax and/or blinatumomab to usual chemotherapy for treating infants with newly diagnosed acute lymphoblastic leukemia (ALL) with a KMT2A gene rearrangement (KMT2A-rearranged \[R\]) or without a KMT2A gene rearrangement (KMT2A-germline \[G\]). Venetoclax is in a class of medications called B-cell lymphoma-2 (Bcl-2) inhibitors. It may stop the growth of cancer cells by blocking Bcl-2, a protein needed for cancer cell survival. Blinatumomab is a monoclonal antibody that may interfere with the ability of cancer cells to grow and spread. Chemotherapy drugs work in different ways to stop the growth of cancer cells, either by killing the cells, by stopping them from dividing, or by stopping them from spreading. Adding venetoclax and/or blinatumomab to standard chemotherapy may be more effective at treating patients with ALL than standard chemotherapy alone, but it may also cause more side effects. This clinical trial evaluates the safety and effectiveness of adding venetoclax and/or blinatumomab to chemotherapy for the treatment of infants with KMT2A-R or KMT2A-G ALL.
This study is being done to answer the following question: can the chance of prostate cancer growing or spreading be lowered by adding a drug to the usual combination of drugs?
This study would like to find out if this approach is better or worse than the usual approach for prostate cancer.
The usual approach for patients who are not in a study is hormone treatment with Androgen Deprivation Therapy (ADT) and Androgen-Receptor Pathway Inhibitor (ARPI).
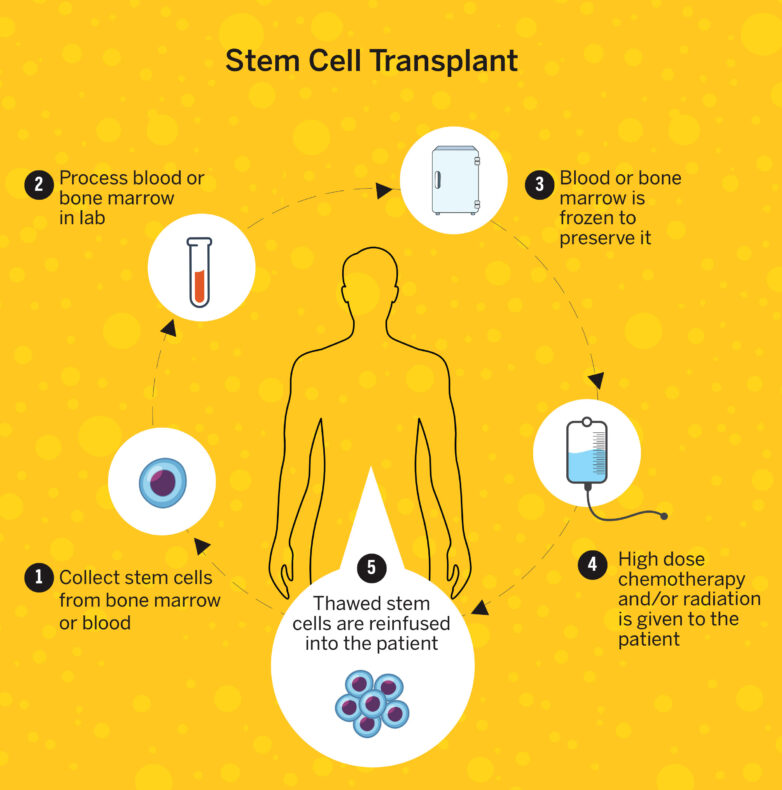
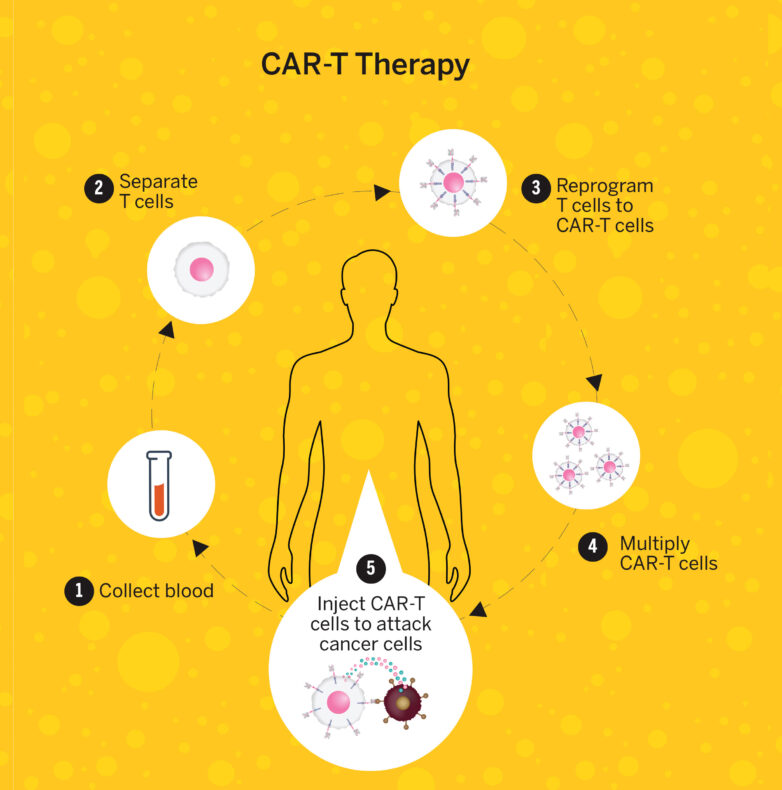
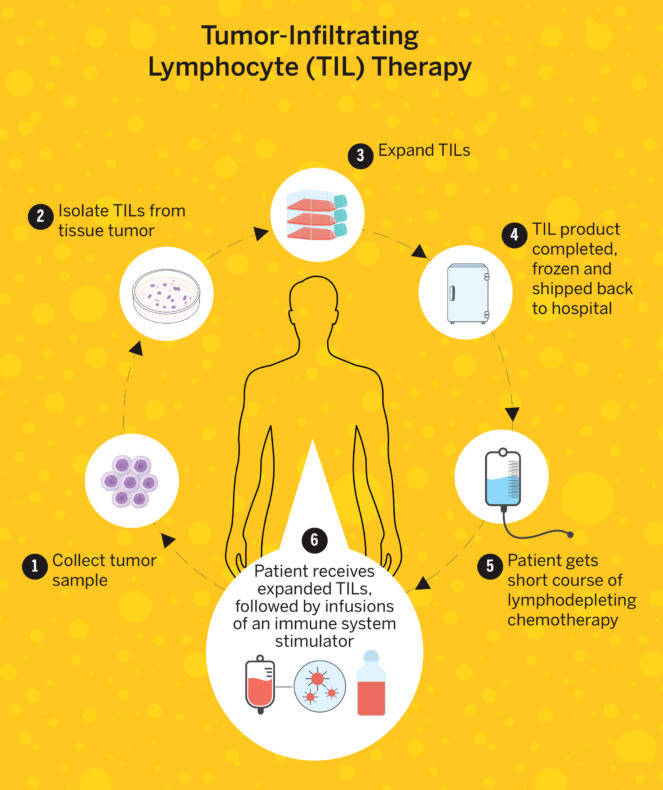
There are many types of cellular therapy. Vanderbilt-Ingram has one of the nation’s best stem cell transplant centers based upon procedure volume and patient outcomes. The center was the first in Tennessee to offer CAR-T (chimeric antigen receptor T cell) therapy, which reengineers a patient’s immune cells to recognize and attack cancer. Another cellular therapy Vanderbilt-Ingram recently added is TIL (tumor-infiltrating lymphocyte) therapy for advanced melanoma. TIL became the first cellular therapy approved by the Food and Drug Administrations for solid tumors in February 2024.
In the summer of 2021, I was diagnosed with Stage 4 renal cell carcinoma. Needless to say, my world was turned upside down. Cancer is such a devastating disease, and no one wants to be a part of that club. No preplanning for this one. Yet, there I was, handed this diagnosis with no plan in hand.
“What’s next?” I thought. While the radiologist was giving me some direction on my recent discovery, I totally passed out! “This couldn’t be happening, could it? Look at me, I’m a healthy, physically fit, soon to be retired happy-go-lucky male.” Ironically, in all of this, I just received my very first Social Security deposit earlier that morning. Good luck seeing my next one!
Two weeks later, I was undergoing a serious operation to remove my right kidney and 11 centimeter tumor when the unimaginable happened. Parts of the tumor broke apart during the resection. A loose thrombus from the large tumor traveled up my inferior vena cava and into my heart, which stopped my blood flow for up to 10 minutes. That generally means instant death! Obviously, I didn’t “expire,” as I am here writing this dialogue for you. However, there are many excruciating details of how I ultimately survived that surgery and lived to talk about it. That particular incident and my cancer journey that followed are quite a story. In fact, I authored a bestselling book describing that operation and what really happened in those 10 “lifeless” minutes.
The book recounts that major event along with the six months that followed. It was quite a ride enduring the cancer emotions for both me and my wife along with the continual cancer treatments. My therapy following the operation involved a regimen of pembrolizumab infusions, which is an immunotherapy, along with a daily intake of Inlyta pills, a targeted therapy that inhibits the growth of cancer cells.
After following this schedule for the two years that was prescribed, it was decision time. I had great success with the mix of these two drugs in fighting my cancer, although I encountered many side effects along the way. I was determined to stay the course no matter what the consequences were. Now at this crossroad, I had many options to consider. Keep the medication intake the way it was? Reduce the number of medications? Or a combination of many other variables? After giving this much thought, I asked my oncologist at the Medical University of South Carolina, Dr. Theodore Gourdin, about getting another opinion. Dr. Gourdin was gracious regarding my question and suggested two other oncologists who specialized in kidney cancers. One of the doctors he mentioned was Dr. Brian Rini at Vanderbilt-Ingram Cancer Center in Nashville. I researched Dr. Rini online and felt like he was my guy. After all, he had authored the treatment study that I’d been on for the past two years.
Hollings Cancer Center at the Medical University of South Carolina contacted Vanderbilt-Ingram and introduced me to them in order to get the ball rolling. I followed their introduction with a call to set up an appointment. I was impressed from the moment the receptionist answered the phone. She was very welcoming, and after some discussion she switched me over to Dr. Rini’s navigator who was already familiar with my case. She scheduled an appointment for a Thursday at 10 a.m. That was only 48 hours from the time I was speaking to her.
I would need to step it up as the cancer center was over 500 miles away involving an eight-hour-plus drive. We would have to leave early Wednesday morning to arrive in Nashville at a reasonable hour. Considering that MUSC and VUMC used the same software company, (Epic Systems Corp.), I was able to merge the two systems so Dr. Rini would have immediate access to all my medical records. It was amazing how all of this came together in short order.
William and Linda Douglas take a stroll on the beach with their standard poodle, Gianni.
My wife, Linda, and I, along with our standard poodle, Gianni, loaded up our SUV Wednesday morning and headed toward Nashville. Ingram Content Group, the company that would print my book on cancer is located in La Vergne, Tennessee, southeast of Nashville. Considering it was along the way, I thought it would be beneficial to stop and see the facility that would ultimately publish my book when it came out. This trip was kind of full circle for me, being that the cancer center that I was heading to was named in honor of the family who made a large contribution to Vanderbilt University Medical Center for the cancer center. This was all very surreal to me in a good way.
We arrived in Nashville on Wednesday evening and checked into a hotel near the Vanderbilt campus. After unpacking, we drove around the college campus and noted the beauty of it all. We found the cancer center and parked our car in the convenient parking garage adjacent to the large glass building. I had Linda take my picture next to the Vanderbilt-Ingram Cancer Center sign located in front. We noticed that they had complimentary valet parking. We thought that was a nice offering, but we would forgo that service the next morning. After finding a good barbecue restaurant that evening, we went to bed with great anticipation for my appointment the next morning.
We woke up early and took Gianni for a nice stroll in the downtown area. Nashville is a very friendly town that displays country music everywhere you look. The downtown atmosphere was relaxing and a joy to walk through. After our short dog walk, we got Gianni situated in our motel room and headed to our appointment with Dr. Rini.
When we walked into the lobby of the cancer center, I immediately noticed the piano situated against the paneled wall of the room. It was a shiny black piano that had a calming appearance to it. It all made sense being we were in Nashville.
The flooring was carpeted, with comfortable seating scattered throughout the spacious room. I took note of the coffeepot on the self-service bar that I thought was a nice touch. It was obvious that Vanderbilt went to great lengths to make its cancer patients feel comfortable while visiting their oncologists. We checked in with the nice lady at the front desk, who entered my information into their system, then we took a seat in the lobby. It was approximately 10 minutes to 10 a.m. when Dr. Rini’s nurse called my name. “That didn’t take long,” I thought. We followed her to the exam room, where she asked a few questions and said that Dr. Rini would be in shortly.
At precisely 10 a.m., Dr. Rini entered the room. He didn’t have a medical chart, laptop computer or anything such as this with him. He was sharply dressed; however, he wasn’t wearing the usual white coat that most doctors wear. This created a much more relaxing atmosphere. We shook hands; he introduced himself; and we all took a seat.
He looked me in the eye and said, “I have studied your case and know it very well. Your situation is very unique, and I’m glad you’re doing so well after a rocky start to your journey.” We jumped into some particulars regarding my nebulous cancer outlook. I was very impressed that he didn’t have to refer to any notes on the topics we discussed. After a 30-minute conversation, we jointly came to a satisfactory conclusion as to how I needed to proceed going forward. As we exited the exam room, Dr. Rini said he would keep up with my progress and to never hesitate to reach out to him if I felt the need to do so. I felt comfort in knowing that.
As I exited the Frances Williams Preston Building, I turned around, took a good look and thought, I know I came to the right place, at the right time, and saw the right doctor. This is probably the most satisfied feeling I’ve had since my cancer diagnosis. To have the validation from this wonderful cancer facility along with the work that my magnificent cancer center in Charleston has already accomplished, I couldn’t be in a better place. I’m very fortunate to have been treated by two outstanding National Cancer Institute-designated Cancer Centers, and my success in fighting this terrible disease will be a reflection of that.
The cellular therapy programs at Vanderbilt-Ingram Cancer Center, Monroe Carell Jr. Children’s Hospital at Vanderbilt, and the VA Tennessee Valley Healthcare System have received reaccreditation from the Foundation for the Accreditation of Cellular Therapy (FACT).
Founded in 1995, FACT establishes standards for high-quality medical and laboratory practice in cellular therapies. FACT is a nonprofit corporation co-founded by the International Society for Cell and Gene Therapy and the American Society for Transplantation and Cellular Therapy for the purposes of voluntary inspection and accreditation in the field of cellular therapy.
“FACT is an internationally recognized accrediting body for hospitals that offer stem cell transplant and cellular therapy, and recognition by FACT indicates that the accredited institution has met the most rigorous standard in every aspect of cellular therapy,” said Adetola Kassim, MBBS, MS, professor of Medicine and clinical director of the Adult Stem Cell Transplant Program. “This covers the entire spectrum of stem cell therapy from clinical care to donor management, cell collection, processing, storage, transplant, administration and cell release.”
The Vanderbilt and VA Tennessee Valley Healthcare System programs received accreditation notification April 14 after on-site inspections in October 2024. The accreditation is effective for three years.
Cancers that were once almost always fatal for children are now curable because of advancements in cellular therapies that Vanderbilt-Ingram Cancer Center pediatric oncologists and hematologists have introduced to Tennessee.
The advancements have included improvements for HLA (human leukocyte antigen) matching with stem cell donors, better medicines for infection prevention, new therapies for graft-versus-host disease (GVHD) and CAR-T therapies.
“We were one of the first sites in the state to be able to use CAR-T to treat our patients, and that’s really been a big game changer for some of our patients who had relapsed or refractory leukemia that would have otherwise been fatal,” said Carrie Kitko, MD, Ingram Professor of Pediatric Oncology and medical director of the Pediatric Stem Cell Transplantation Program.
The program has established itself as a leading innovator in preventing and treating GVHD, which occurs when donor immune cells begin attacking the stem cell recipient’s healthy tissue. Vanderbilt-Ingram is part of an international consortium called MAGIC that has developed risk-stratified treatments according to both GVHD symptoms at presentation and biomarkers, or certain proteins in their blood, to predict patients who are more or less likely to respond to treatments for GVHD.
“We have had several clinical trials to potentially improve outcomes for patients with GVHD. If you’re a low-risk patient, we’ve been able to offer trials where we avoid steroids, which are normally what we use to treat our GVHD patients, but steroids have lots of side effects that can be quite unpleasant,” Kitko said.
“You can identify those low-risk patients that don’t need steroids, and you can use a less toxic therapy. And then for the high-risk patients, if we know that they’re unlikely to respond to steroids, why wait for them to fail on steroids. We have been able to offer some of these studies to both pediatric as well as adult patients.”
Kitko is the senior author of a study published in 2024 in The New England Journal of Medicine that led to the Food and Drug Administration approving a new drug for recurrent or refractory chronic GVHD. Patients who were given the drug, axatilimab, had an overall response rate of 74%.
“Now, patients have access to more drugs to treat chronic GVHD, which is really a very morbid condition for many of our patients,” she said. “Moderate to severe chronic GVHD really impacts their quality of life and their ability to do normal day-to-day activities.”